Irresponsible Drinking & Regulation
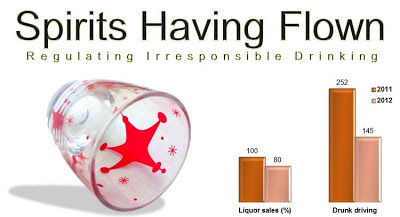
Irresponsible drinking requires regulation to modulate its potential for harm. There are specific neurotoxic effects of alcohol drinking . The responsible individual needs to learn personal skills to refuse alcohol drinking when required to do so. The potential harm to society with irresponsible drinking and driving necessitates regulation at a societal level. Regulating irresponsible drinking Alcohol drinking and driving in Pune over New Year's eve was markedly reduced as compared to last year. This year 145 drunk driving arrests were made as against 252 last year. This reduction was despite an increase in the total number of arrests made in Pune for irresponsible drinking and driving in 2012 as compared to the previous year. The heightened deployment of police personnel manning 30 prominent points of the Pune roads on New Year's eve was apparently deterrent enough. Alcohol drinking and liquor sales were down by 20-30% in S...
