Adult ADHD - Attention Deficit Hyperactivity Disorder at work
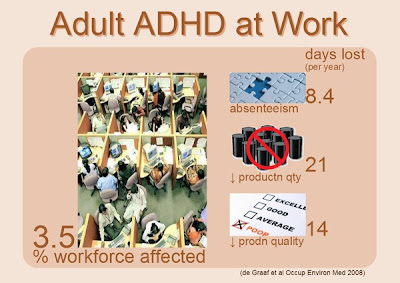
ADHD (Attention Deficit Hyperactivity Disorder) is thought to be a childhood disorder. However ADHD persists in adults in up to 50% of children diagnosed with the disorder. Hyperactivity, impulsivity and inattention; the hallmark symptoms of Attention Deficit Disorder in childhood have been described earlier. In Adult ADHD, symptoms change to reflect the child's development into adulthood. The symptoms related to hyperactivity gradually disappear by adulthood; however, those related to inattention persist. Adults with attention deficit disorder (ADD) are often distracted, and avoid tasks requiring sustained mental effort. This impairs functioning at home and at work. Adult ADHD at work Adults with ADHD experience employment impairments at every level; from the initial job search, to the interview and then during the employment itself. People with Attention Deficit Disorder are more likely to be have poor job performance, l...
