 |
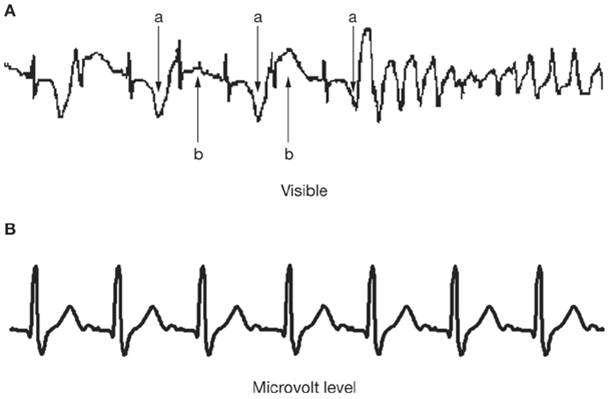
| Anger induced electrical changes in the heart |
Why we need the emotion of anger
Charles Darwin was the first to note the universality of anger and other facial expressions of emotion. He viewed this as evidence that emotional signals like anger have been stamped by evolution into the central nervous system. Anger has an essential survival function. Anger needs to be controlled or managed for it to be effective.Anger management strategies
These are strategies to change your attitude to the expression of anger, as also immediate and long term behaviours to control anger.Focus and mindset strategies
To control anger one needs to control the scripts that lead up to it- He's being stupid again. Recognise how easy it is for the best among us to be wrong and make mistakes. Don’t expect life to go on as planned
- It's OK to blow my top once in a while. Talk things over before you reach the explosive stage. Think of how you will regret having been indiscrete and hurting someone. It could work to your disadvantage later. Don’t view an occasional outburst as good for letting off steam. Don’t bottle up your feelings - express them civilly.
- I'll show him who's boss. Remember that your aggression is likely to spark a chain reaction of aggression in others. Losing your temper is not the mark of a strong character who knows his/her mind
- That's my right. There is a difference between feeling indignation and losing your temper because you cannot have things your way. The former leaves room for negotiation, the latter only makes things worse
Strategies for immediate anger control
- Monitoring your feelings is one of the key skills for anger control. Be aware of your body sensations, such as flushing, muscle tensing, and heart beat as you are getting angry. Take those feelings as a cue to stop and consider what to do next instead of shouting or lashing out.
- Force yourself to keep your voice down. Make a deliberate attempt to speak quietly and slowly
- Take 'time out'. Remove yourself physically by walking away from the place of argument
- Count to ten slowly so the impulse to retort will pass
- Look at your face in the mirror. Now you know why the others are laughing
What to do in the long run
Study your anger. Keep a diary of trigger incidents. Look for the pattern. Avoid precipitating situations as far as possible. Two situations that commonly precipitate anger.- Insecurity, which makes you unduly sensitive. Social cues interpreted as hostile may in fact be neutral or friendly
- Frustration. Learn to accept what can’t be altered. Do your best – do not frustrate yourself over what is not in your control.
Understand people who make you angry. Ask yourself: ‘why do I always get angry with him/her?’ Why do you find them irritating? Enter into their experience – what does it feel like to be them? Others may not accept your point of view all the time. Understand the other person’s point of view. Don't be judgemental.
Relax. Incorporate a relaxation period in your routine – meditation, yoga, music; whatever works for you.
Get direct training in anger control. Many individuals are unhappy that they lose their temper easily. They are receptive to learning how to control it. In the heat of the moment, cool-headed responses such as walking away or counting to ten so the impulse to hit will pass are not automatic. Practice such alternatives in role-playing scenes. Try out friendly responses that preserve dignity while giving an alternative to shouting, hitting, and sulking.
Anger may signal a treatable underlying mood disorder. Treat it. Protect your heart
References
- Eric J. Rashba . Anger Management May Save Your Life: New Insights Into Emotional Precipitants of Ventricular Arrhythmias. J. Am. Coll. Cardiol. 2009;53;779-781. doi:10.1016/j.jacc.2008.11.023
- Rachel Lampert, Vladimir Shusterman, Matthew Burg, Craig McPherson, William Batsford, Anna Goldberg, and Robert Soufer. Anger-Induced T-Wave Alternans Predicts Future Ventricular Arrhythmias in Patients With Implantable Cardioverter-Defibrillators. J Am Coll Cardiol, 2009; 53:774-778, doi:10.1016/j.jacc.2008.10.053




{kind=link}