 |
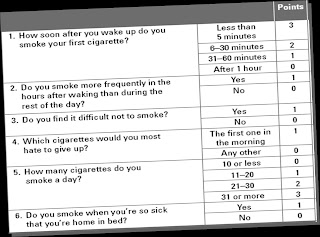
| Fagerstrom Test for Nicotine Dependence |
Quitting tobacco is the most important thing you can do to protect your health
(AHRQ)
Quitting by willpower only
40% of smokers try to quit each year. The success rate of those who quit on their own is about 5% and with self-help books it is about 10%. Most smokers make 5-10 attempts to quit. Unsuccessful attempts to quit are a sign of nicotine dependence.85% of current daily smokers are nicotine dependent
Signs of nicotine dependence
- Tolerance - Increasing the number of cigarettes smoked per day (Most smokers escalate to a pack)
- Withdrawal - Mood changes, irritation, anxiety, insomnia, restlessness when unable to smoke
- Loss of control - Most smokers do not intend to continue, but 5 years later 70% do
- Increased time spent using the drug - Leaving office/ work-site to smoke
- Continued use despite harm - cough, hypertension, heart disease
- Giving up important activities - air travel
Are you nicotine dependent?
Take the Fagerstrom TestYou can quantify the extent of your dependence by adding your points scored for each question.
- 7-10 points - high level of addiction
- 4-6 points - medium level of addiction
- 0-3 points - low level of addiction
Why does nicotine produce a severe dependence?
- Nicotine has direct effects on concentration and mood
- Nicotine reaches brain in seconds → a rapid effect
- Allows user to titrate the dose by varying puff frequency and depth
- The habit is Intense (>200 puffs/day x 20 years)
- There are many environmental cues (eg, others smoking/ ads)
- Never impairs the user via intoxication
How do I quit?
Make a START
Set a quit date-today! Choose a birthday, wedding anniversary, New Year’s DayTell family, friends and co-workers – Enlist their support
Anticipate challenges- Withdrawal symptoms and craving will occur. Tell yourself that you can face the challenges ahead. Behavioural techniques will help you through this phase.
Remove cigarettes and all related products-lighters, matches, ashtrays from your home and workplace
Talk to your doctor – Medication, Behaviour therapy and Nicotine Replacement Therapy are the mainstay of treatment. Your doctor will help you decide what suits you.
After quitting
The habit is still latent after you have quit tobacco smoking. Some vigilance is required to stay quit. However, the longer you stay quit the easier it becomes. Some of the things you could do to reduce the chances of a relapse are as belowWatch out for the triggers
- Habit situations (things you used to do while smoking)
- Stress / -ve moods
- +ve moods/ celebrations
- Alcohol
- Use coping skills to beat the urge and handle craving
Avoid smoking at all costs
- If you do slip ACT!- QUIT IMMEDIATELY
- Can I have just one cigarette? You must do everything you can to avoid that first cigarette
9 out of 10 people who have that one cigarette after quitting return to regular smoking.
Enjoy the rewards of quitting!
- Within 20 minutes Heart rate slows towards normal
- 8 hours Carbon monoxide levels drop to normal
- 2 weeks-3months Heart attack risk lessens, lung function improves
- 1-9mths Coughing and breathlessness reduce
- 1 year - Heart disease risk ½ of chronic smokers
- 5-15 years - Stroke risk = non-smokers
- 10 years - Risk of death due to lung cancer same as that of non-smoker
- 15 years - Coronary heart disease risk same as that of non-smoker
References
- Agency for Healthcare Research and Quality
- Centers for Disease Control and Prevention
- Heatherton T, Kozlowski L, Frecker R, Fagerström K: The Fagerström test for nicotine dependence: A revision of the Fagerström tolerance questionnaire. British J Adict 1991, 86:1119-27.



{kind=link}