(or why the 25 year age-bar on alcohol consumption could be reasonable)

Does alcohol have specific neurotoxic effects on the adolescent or young adult brain? This question is the only important one for deciding whether the 25 year age-bar on alcohol consumption in Maharashtra is justifiable. While the debate rages two students from the premier medical college of India drowned in an alcohol fuelled swimming pool misadventure, and in an unrelated incident on the same night five inebriated youths were arrested for disturbing the peace in a residential area. We have seen how to recognise problem alcohol drinking in teenagers, and how to refuse alcohol. This article probes the specific effects of alcohol on the maturing brain.
These adverse effects specifically impact the frontal lobes of the brain and are highly associated with level of intelligence. In addition the brain area essential for working memory (hippocampus) is preferentially damaged by alcohol (De Bellis 2000). Gender effects render female adolescents more vulnerable than males to these alcohol effects.
The reward system of the brain is responsible for motivation and learning. The immature reward system has an adolescent-specific vulnerability for alcohol and drug addiction. Early exposure to alcohol sensitises the brain regions involved in drug addiction and alters gene expression in the brain reward regions (nucleus accumbens).
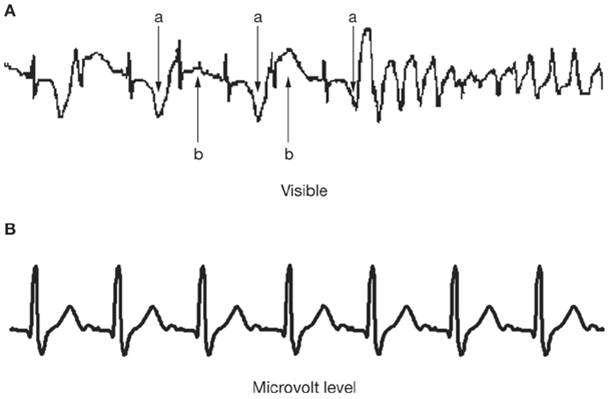
The pattern of brain electrical activity changes during the transition from adolescence to adulthood. Alcohol also has a premature aging effect on brain electrical activity during wakefulness and sleep. Animal models have shown that even brief exposure to alcohol in adolescence can cause long lasting changes in brain electrical activity. These changes place the adolescent at a high risk for later substance abuse and addiction (Ehlers 2010).
Whether the authorities considered the neurotoxic effects of alcohol while imposing the 25 year age-ban on alcohol consumption is a moot point. However, educating adolescents and youth regarding these adverse alcohol effects should be the duty of every parent.
References

Does alcohol have specific neurotoxic effects on the adolescent or young adult brain? This question is the only important one for deciding whether the 25 year age-bar on alcohol consumption in Maharashtra is justifiable. While the debate rages two students from the premier medical college of India drowned in an alcohol fuelled swimming pool misadventure, and in an unrelated incident on the same night five inebriated youths were arrested for disturbing the peace in a residential area. We have seen how to recognise problem alcohol drinking in teenagers, and how to refuse alcohol. This article probes the specific effects of alcohol on the maturing brain.
Infancy
Alcohol is a neurotoxin. It distorts the normal architecture of the developing brain. This distortion starts during pregnancy when imbibed maternal alcohol crosses the placenta into the foetus. In the foetus alcohol acts on the specially vulnerable immature insulating cells (oligodendroglia) of the brain. The child is born with Fetal Alcohol Syndrome, characterised by irreversible mental retardation, a small head, small stature and facial abnormalities. Because the exact amount of alcohol required and the most vulnerable periods of pregnancy have not been definitively established all pregnant women are advised to abstain from any use of alcohol.Childhood
By the second year of life the number of connections between brain cells (synapses) are at a maximum. These synapses are gradually reduced to the adult number (synaptic pruning). This process is controlled by immature excitatory (glutamate) receptors in the synapses. These receptors differ from adult ones by allowing quicker and longer excitation. Immature glutamate receptors are vulnerable to the effects of alcohol. Their over-stimulation distorts synaptic pruning (Johnston 1995).Adolescence
In adolescence there is a rapid growth of gray matter and the formation of new connections (proliferation) in the brain. Elimination of some synaptic connections (pruning) enables the adolescent or young adult brain to change in response to environmental demands. Stability of these connections is enhanced through insulation of neuronal fibres (myelination). Myelination increases the overall speed of information processing within the brain. These maturational processes are critical for cognitive development. They are all adversely affected by alcohol (Guerri 2010).These adverse effects specifically impact the frontal lobes of the brain and are highly associated with level of intelligence. In addition the brain area essential for working memory (hippocampus) is preferentially damaged by alcohol (De Bellis 2000). Gender effects render female adolescents more vulnerable than males to these alcohol effects.
The reward system of the brain is responsible for motivation and learning. The immature reward system has an adolescent-specific vulnerability for alcohol and drug addiction. Early exposure to alcohol sensitises the brain regions involved in drug addiction and alters gene expression in the brain reward regions (nucleus accumbens).
The pattern of brain electrical activity changes during the transition from adolescence to adulthood. Alcohol also has a premature aging effect on brain electrical activity during wakefulness and sleep. Animal models have shown that even brief exposure to alcohol in adolescence can cause long lasting changes in brain electrical activity. These changes place the adolescent at a high risk for later substance abuse and addiction (Ehlers 2010).
Youth
Alcohol differentially impairs the young persons judgement and motor skills. The evidence for this is so robust that some administrations have placed a lower legal blood alcohol level limit on drivers less than 21 years old (Hingson 1994). This differential susceptibility to alcohol has been shown to persist up to 30 years of age when a specific impact is seen on frontal lobe functions related to driving skills (Domniques 2009).Whether the authorities considered the neurotoxic effects of alcohol while imposing the 25 year age-ban on alcohol consumption is a moot point. However, educating adolescents and youth regarding these adverse alcohol effects should be the duty of every parent.
References
- De Bellis MD, Clark DB, Beers SR, Soloff PH, Boring AM, Hall J, Kersh A, Keshavan MS. Hippocampal volume in adolescent-onset alcohol use disorders. Am J Psychiatry. 2000 May;157(5):737-44.
- Domingues SC, Mendonça JB, Laranjeira R, Nakamura-Palacios EM. Drinking and driving: a decrease in executive frontal functions in young drivers with high blood alcohol concentration. Alcohol. 2009 Dec;43(8):657-64.
- Ehlers CL, Criado JR. Adolescent ethanol exposure: does it produce long-lasting electrophysiological effects? Alcohol. 2010 Feb;44(1):27-37.
- Guerri C, Pascual M. Mechanisms involved in the neurotoxic, cognitive, and neurobehavioral effects of alcohol consumption during adolescence. Alcohol. 2010 Feb;44(1):15-26.
- R Hingson, T Heeren, and M Winter. Lower legal blood alcohol limits for young drivers. Public Health Rep. 1994 Nov-Dec; 109(6): 738–744.
- Johnston MV. Neurotransmitters and vulnerability of the developing brain. Brain Dev. 1995 Sep-Oct;17(5):301-6.







{kind=link}
{kind=link}